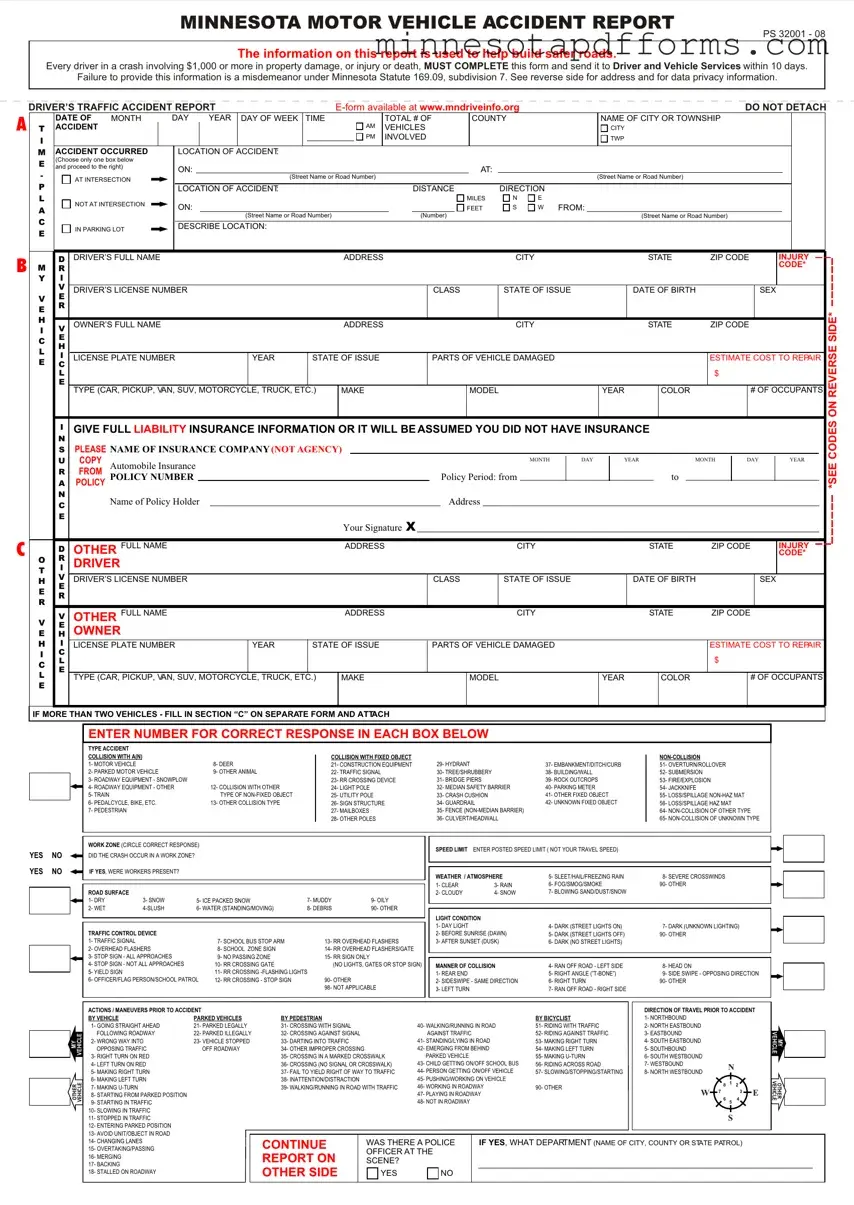
The Minnesota Motor Vehicle Accident Report form shares similarities with other official reports and documentation used in various sectors and circumstances. These documents, while tailored to their specific contexts, follow a general pattern of collecting detailed information for the purpose of analysis, accountability, regulation, or law enforcement. Below are nine documents that are similar to the Minnesota Accident Report form in their structure and purpose.
One example is the Police Incident Report, used by law enforcement to document the details of a crime or incident. Like the accident report, it gathers comprehensive information about the parties involved, the location, and the specifics of the event. This information is crucial for both the investigation process and as a record for future reference.
Another related document is the Workers' Compensation Claim form. Workers who get injured on the job fill out this form to report the incident. It captures personal information, details of the injury, and circumstances leading to the incident, paralleling the structured data collection seen in the accident report to determine eligibility for compensation benefits.
Similarly, the OSHA (Occupational Safety and Health Administration) Accident Report form is used in workplaces to report incidents that result in injury, illness, or death. This form helps in analyzing workplace safety and health conditions, underlining the importance of gathering detailed accounts of incidents, akin to the vehicle accident report’s role in road safety analysis.
The Insurance Claims Form is also akin to the accident report, as it is used by policyholders to report incidents covered by their insurance policy. It collects detailed information about the incident, damage, and parties involved, essential for claim processing and determination of liability or coverage, illustrating the focus on contractual and financial accountability similar to assessing road incidents.
A Flight Incident Report, used by the aviation industry, records occurrences on board or involving aircraft that may affect safety. Much like the road accident report, it compiles comprehensive details about the incident to improve future safety protocols and for regulatory compliance.
The Maritime Accident Report, used for incidents at sea, collects exhaustive information about maritime accidents, including vessel details, crew information, and the sequence of events leading to the incident. This detailed documentation aids in enhancing maritime safety and navigating regulatory requirements, mirroring the road accident report's objectives on waterways.
Another comparable document is the FDA (Food and Drug Administration) Adverse Event Reporting form, which documents adverse reactions or quality issues with FDA-regulated products. This form's systematic collection of detailed incident information is vital for public health safety, akin to how accident reports support road user safety.
The Product Safety Complaint form, used by consumers to report unsafe products, also shares similarities. It details the product fault, the incident, and any injuries, providing essential data for safety standards and recalls, emphasizing the role of detailed reports in consumer protection, like the accident report's role in vehicular safety.
Lastly, the Environmental Incident Report form, used to document incidents impacting the environment, like pollution or wildlife disturbances, collects details about the incident's nature, cause, and effects. This parallels the accident report's goal of collecting data to prevent future occurrences and manage risks, focusing on environmental protection.
Overall, while each document serves a specific sector or purpose, their fundamental similarity lies in their structured approach to gather detailed and specific information following incidents. This data collection is crucial for analysis, decision-making, policy formulation, and enforcement in their respective fields, much like the Minnesota Motor Vehicle Accident Report form's role in road safety and legal compliance.